
Quantifying Payer Decisions: A Structured Approach to a “Small Sample” World
"We can't quantify this. The samples are too small." It's one of the most persistent yet limiting assumptions in payer research.
The assumption usually stems from a mismatch: applying consumer research logic to a fundamentally different kind of decision. In payer research, small samples aren't disqualifying. They're a design constraint. Respect that constraint, and you can model payer decision-making with surprising clarity.
Payers don’t behave like consumers. They’re not choosing between flavors of yogurt or comparing lifestyle brands. They’re making structured, financially anchored decisions inside a system with clear incentives and well-understood levers. When the decision environment is structured, the noise drops. You don’t need hundreds of respondents to detect a signal that’s already strong; you just need a disciplined design.
That’s why ordered choice modeling works so well in this application. Formulary outcomes such as tier placement, restrictions, coverage aren’t random categories. They form a natural hierarchy. When you treat them as an ordered system rather than a set of disconnected boxes, you can quantify how pricing, rebates, clinical differentiation, and competitive context shift the likelihood of each access outcome.
The key lies in maintaining discipline: focusing on fewer attributes, defining sharper levels, emphasizing real contracting levers, and avoiding any decorative variables (variables that sound important but don't actually predict outcomes). When you design the exercise around what truly drives payer decisions, the model becomes both stable and interpretable. And because the output is probabilistic, you can translate it directly into the language that matters: the share of covered lives likely to receive each level of access.
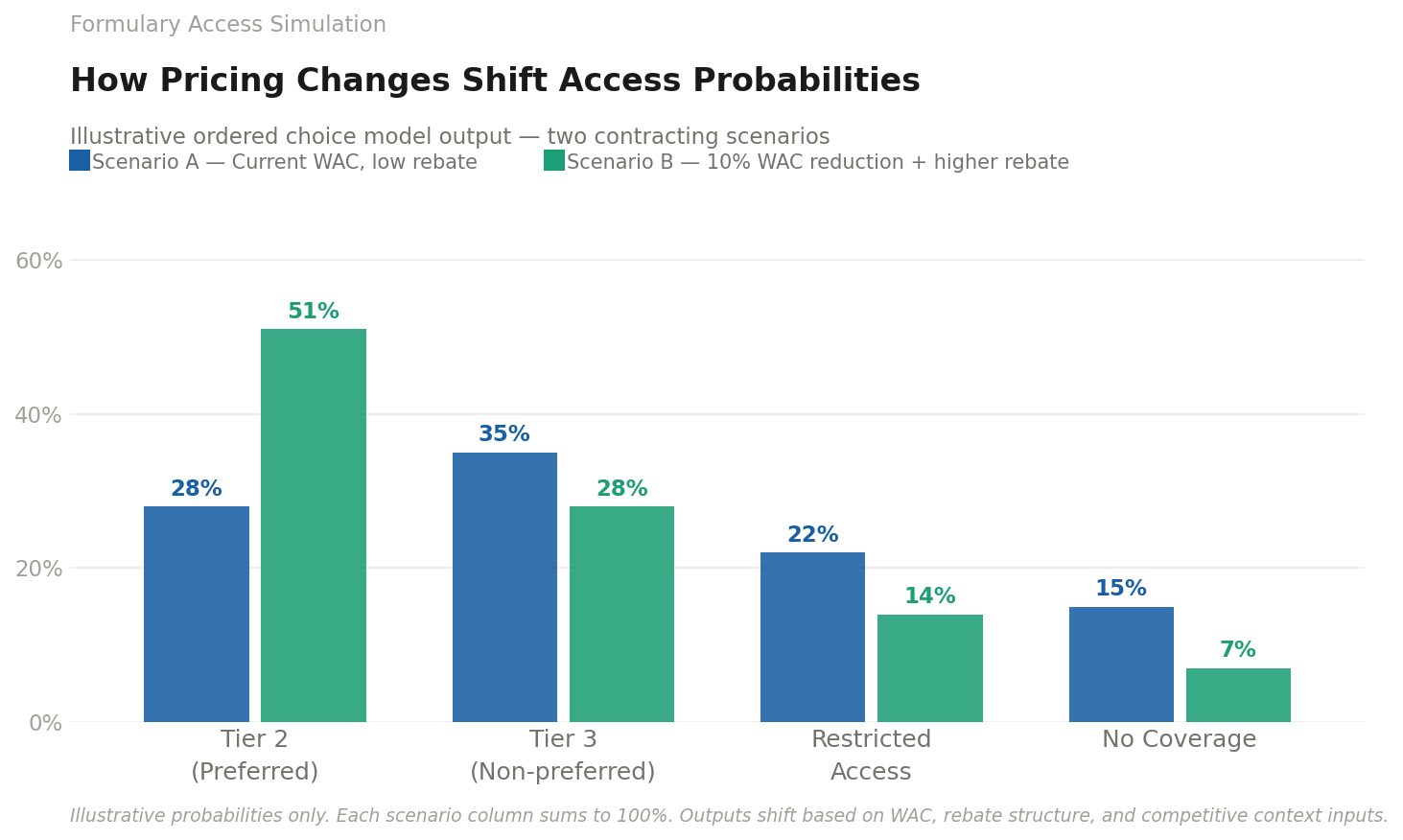
This is where the simulator becomes powerful. Once you have a model that produces access probabilities, you can build a tool that lets teams explore “what if” scenarios—pricing moves, rebate structures, competitor entries, indication expansions. It becomes a workspace for decision-making, not a static deliverable. You can see how a 10% WAC change shifts Tier 2 access. You can test contracting strategies before you take them into the market. You can pressure-test launch assumptions with something more rigorous than intuition.
And this matters more now than it did even a few years ago. PBM consolidation has created more uniform policy structures. Net price transparency is increasing. Pre-launch access forecasting is no longer optional. Value-based contracting is expanding. In this environment, qualitative insight is still essential—but it’s not enough on its own. Teams need structured, probabilistic views of how payers will respond to the choices they’re considering.
Small samples don’t hinder our ability to quantify; instead, they sharpen our focus. They compel us to eliminate distractions and concentrate on the levers that truly influence outcomes.
If your team is still treating payer research as inherently qualitative, it may be worth reconsidering what structured design can do in a quantitative setting.